Плавание
Огромное спасибо xasm за ссылку на отличную статью http://early-onset-scoliosis.com/Documents/Scoliosis%20in%20Swimmers.pdf
Scoliosis in Swimmers
Theodore. Becker, Ph.D" R.P.T., A.T.C'* (Member of the United States Swimming Sports Medicine Committee Executive Council and International Teams Staff 149CLinics in Sports Medicine-Vol. 5, No. I, January 1986)
Children who become interested in swimming and begin to participate seriously often do so at very early ages, sometimes as young as six or seven. This early involvement very often exposes them to types of stress that can affect the growth and development of their maturing musculoskeletal systems in an adverse way, producing a disruption of the normal growth pattern, The most potentially serious of these growth disorders is scoliosis of spinal curvature, because it may deform the body and inhibit normal bodily organ function.
FUNCTIONAL AND STRUCTURAL SCOLIOTIC CURVATURE
The vertebral curvature that is defined as scoliosis has been broadly categorized as either structural or functional. The structural curvature category has been described by Willner [34] Hauser [14] and Portillo [23] as being a deviation of over 10 degrees, accompanied by rotation. This definition specifies the inclusion of bone and ligament malfunction as a criterion for structural torsion associated with a lateral curvature.
Functional scoliosis has been referred to by Keim [16] as a "mild" form of the vertebral disorder, because it is not necessary to correct the condition by an external device, but rather it can be corrected by side bending.
Arkin [3] further noted that the functional or mild curve may in some cases be an initiating cause of the more severe structural curvature, but it is notably a postural fault for which correction is possible without surgery.
Tachdjian [30] noted that functional scoliosis generally has a single long thoracolumbar curve with a predominately left convexity. His work indicates functional scoliosis produces little rotation of the vertebral body with accompanying rib deformity, which is the serious secondary complication of idiopathic scoliosis.
One of the characteristics of functional scoliosis is that the curve will disappear during recumbency and suspension, and the spine bends equally well to both sides on lateral flexion of the trunk, with rotation to both sides being equal. According to Tachdjian [30] the majority of functional scoliosis cases are attributable to compensatory lower limb growth, or compensatory pelvic tilt adjustments affecting the lumbosacral junction. Some degree of functional scoliosis is a common occurrence with poor posture, but this entity is of little clinical importance and ordinarily requires no treatment.
INCIDENCE OF SCOLIOSIS
The incidence of idiopathic structural scoliosis has been normally low among the general population, but is notably higher among adolescents. In a 1955 survey of 50,000 adolescents in the general population, Shands and Eisberg [28] found 1.9 per cent or approximately 1000 subjects to have scoliosis. Avikainen and Vaherto [4] in 1983 reported scoliosis to be present in 3 to 16 per cent of the population, depending on the degree of curvature that had been chosen as the limit of scoliosis, and on the age of the subject. These percentages are similar to the findings of Willner [34] who in 1984 reported 0.35 to 13 per cent as the incidence ofstructural scoliosis. Eckerson and Axelgaard [ll] in 1984 also reported that idiopathic scoliosis, with a lateral curvature of unknown etiology, comprises 75 to 80 per cent of all scoliosis in the United States.
Studies focusing on the incidence among men and women include the work of Shands and Eisberg [28], which showed a predominance among women; the incidence of scoliosis may be five times as great as that found in like male population.
Avikainen and Vaherto [4] report in all cases of scoliosis requiring treatment, 90 per cent are women, but mild scoliosis observed to be nearly as frequent in boys as in girls. Other investigations by Wynne-Davies [36] and Fisher and DeGeorge [12] surveyed familial incidence of scoliosis and the relationship to mothers’ age. These studies showed a significantly greater than expected number of scoliotic curvatures among the offspring of mothers who were considered to be older. In additional investigations, Yarom, Wolf, and Robin [27] indicated that growth and sex hormones and scoliotic onset later in life may be decisive factors in the propagation of the deformity.
Further work on the incidence of scoliosis reported by Kuprian, Ork, and Meissner [18] indicates that Jenschura found the average frequency if idiopathic scoliosis in athletes to be 2 per cent. Krahl and Steinbruck [17] in examining 571 top athletes in 1974-1977, found a 33.5 per cent incidence of functional scoliosis and a 1.6 per cent incidence of idiopathic scoliosis, similar to the incidence noted by Shands and Eisberg [28]. Kuprian, Ork, and Meissner [18] postulated that the high incidence of functional scoliosis among athletes is notable among those participating in sports that develop extreme torque in repetitive serving, throwing, and volleying motions, such as archers, javelin throwers, pole vaulters, and table tennis players.
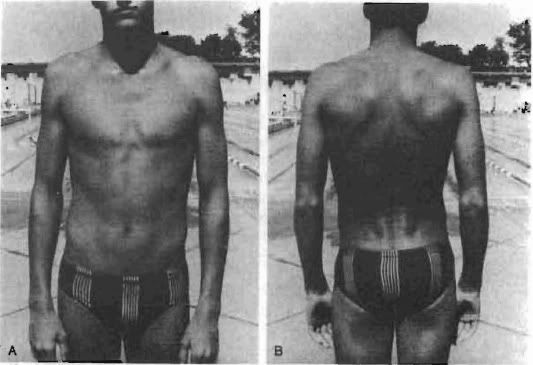
Figure 1. A and B Athletes screened for scoliosis were observed in the standing erect position for asymmetries of the lateral contours of the trunk, shoulders, and scapulae.
The clinically observed scoliosis in swimmers does present the aquatic sports physician and therapist with a potentially interesting investigation as to etiology and incidence. Owing to the great number of adolescents engaged in competitive swimming programs each year, a preliminary study was conducted to ascertain the incidence of scoliosis among this group. In August of 1983, at the Junior Olympic Swimming Championships East, held at the Indiana University Natatorium, Indianapolis. 836 of 1200 competitors underwent evaluative screening for scoliosis. The procedure was patterned after the protocol of Dendy, Chase, and Determann [10], Risser [24], and Willner [34]. This screening procedure included observations with the athlete in the standing erect position, and then in the forward bending position. In the standing erect position, observations were made for asymmetries of the lateral contours of the trunk (Fig 1), shoulders, scapulae, and the lateral deviation of the spinal processes (Fig. 2).
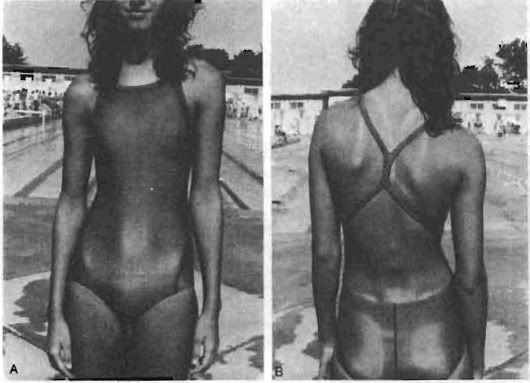
Figure 2. A and B. Swimmers screened for scoliosis were also observed for lateral deviation of the spinal processes.
Of the 336 athletes who participated, 198 females and 173 males, 6.9 per cent were found to have structural idiopathic signs in each group. Each of these groups was found to have a 16 per cent incidence of mild functional scoliosis. The 6.9 per cent figure represents an incidence that is three and one half times the normal incidence, and is well above the 1.9 per cent figure in other studies [17, 28], whereas the 16 per cent is similar to the high figures of Avikainen and Vaherto and of Willner [34] yet below the 33.5 per cent figure of Krahl and Steinbruck [17].
The screening investigation at the Junior Olympic Swimming Championships East, in which 16 per cent were noted to have mild functional curvatures, did produce a unique statistic. In this study the 16 per cent figure included a 100 per cent occurrence of lateral curvature to the hand-dominant side of the body. This supports the muscular imbalance according to Hauser [14], and the dominant arm strength as noted by Yeater et. al. [37], as possible contributors to these particular investigations.
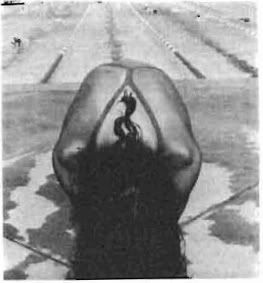
Figure 3. In the forward bending position, observation of rib hump asymmetry was considered to be a positive clinical finding for a structural idiopathic scoliosis.
In the forward bending position, the observed rib hump asymmetry was considered to be the positive clinical finding for structural idiopathic scoliosis (Fig. 3).
It is obvious that the incidence in this small population is of interest to the swimming community, owing to the fact that the event at which the screening clinic was conducted is noted to be a select event. Competitors were entered based on their being capable of swimming at an acceptable level prior to entry, thus placing this population in an elite category, similar to those athletes studied by Krahl and Steinbruck [17].
INTRINSIC EFFECTS OF SWIMMING
It has been stated by Magel and McArdle [21] that the propeling force in swimming depends on muscular strength and eflective stroke mechanics. Swimming speed increases depend in part on buoyancy (плавучесть), the hydrodynamics of correct stroke technique, and wave-making resistance. The propulsive force must equal water resistance, and swimming velocity will result from the relative equilibrium found between force and resistance.
Piette and Clarys [22] electromyographic data revealed the muscles most responsible for the propulsion of the competitive swimmer were the latissimus dorsi, rectus abdominis, gluteus maximus, biceps brachii, and pectoralis. Their investigation revealed the latissimus dorsi, rectus abdominis, and gluteus maximus were the most active muscles during the freestyle stroke. Results of the study showed that competitive swimmers tested had significantly greater propulsion on electromyography than a like number of noncompetitive swimmers. This study also found the muscular efforts of competitive swimmers were significant for the level of activity in the back, abdominals, and muscles of the pelvic girdle.
In succeeding electromyographic studies, Clarys [6] again investigated the latissimus dorsi and rectus abdominis muscles and the results confirmed these to be the most active in duration and strength during the freestyle of all the muscles investigated.
Propulsive efficiency studies by Svec [29] examining the freestyle stroke note the first state of the arm motion produces a pressure curve that is very close to linear from the point of hand entry and pull (Fig. 4A) through to the initial inward scull (Fig. 4B).
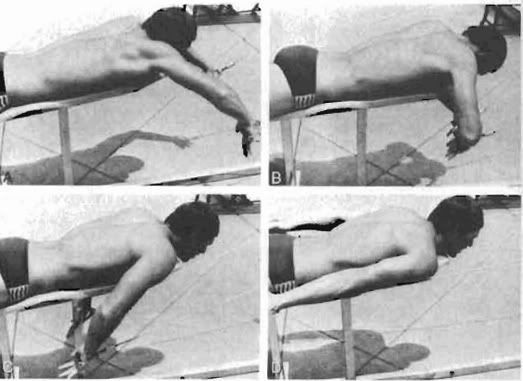
Figure 4. In the freestyle stroke, the first stage of arm motion produces a pressure curve that is very close to linear from the point of hand entry and pull (A) through to the inward scull (B).
The second phone of the stroke, in which pressure curves are greatest, occurs during the last stage of propulsion, when the hand passes the level of the mid chest in the push (C) and finishes in an outward skull phase (D).
The second phase of the stroke, in which pressure curves are greatest, occurs during the last stage of propulsion, in which the hand passes mid chest in the push (Fig. 4C) and finishes in an outward scull phase (Fig. 4D).
High pressure during the propulsive phase of freestyle is almost always present with a duration that is considered to be variable. Yeater et al. [37] in examining the force traces for the crawl stroke, observed that many individuals consistently produced greater peak force with one arm or the other during all phases of propulsion. Quantification of the stroke asymmetry in this study was performed by dividing the right-left differences in peak force by mean peak force, and no appreciable correlation was found between this variable, as well as mean tether force, and competitive velocity.
In another study on the analysis of swimming motions, Gallenstein and Huston [13] found there are dips in the output velocity for all strokes, owing to upper extremity work. Freestyle kicking was noted to produce relatively small changes in the overall freestyle propulsion, and therefore the effort of the upper extremities was interpreted as being relatively unaffected by the efforts of the lower extremities.
Morphologic studies by Sahgal et al. [27] Yarom, Wolf, and Robin [36] and Tachdjian [30] show there are generalized myopathic changes in the paraspinal and gluteus muscles of individuals with idiopathic scoliosis. The structural skeletal changes would then be expected to be accompanied by secondary adaptation of the supporting vertebral soft tissues. The change in soft tissue function is characterized by Tachdjian [30] and Hauser [14] as being atrophy, weakness, and fibrosis on the convex (выпуклый) side of the spine, and thickening and contractions on the concave (впалый) side. (Ровно наоборот. См. http://healthy-back.livejournal.com/178505.html - H.B.)
Of all muscle types tested, [27, 36] there was significant glycogen content, and the mitochondria were found to be significantly higher on the convex side and in the gluteus, but not on the concave side of the apex, where significantly high Z-band values were found.
The histographic work by Yarom, Wolf, and Robin [36] dealt with analysis of the deltoids and the trapezius and quadriceps muscles. These authors reported no striking morphologic pathology, but results of interest included fewer type I Fibers on the concave side than on the convex side. In several cases, the decline was noticeably marked, and the diameters of the fibers were frequently small or hypotrophic, especially on the concave side.
Fiber distribution and size were shown by Yarom, Wolf, and Robin [36] to be clearly characteristic, with a constant decrease in the deltoids of the concave side for the idiopathic sample. The conclusion that was drawn indicated there may be many factors responsible for the noted changes, including intrinsic and hormonally induced membrane abnormalities.
Muscular adaptation has been the focus of several studies by Mass, [20] and Jensen and Bullow [15]. Maas reported the shape of the pectoralis in swimmers was significantly dilierent than in gymnasts, indicating that the sport activity was functionally specific in relationship to the development of the musculature.
Jensen and Bullow [15] report similar information, with evidence that modeling of drag and inertial forces in the freestyle stroke conceivably provide a suffcient load so as to produce functional changes in the muscles, with an expected increase in the contraction moments. This
research additionally found that the contraction moments largely determined the propulsive force of the shoulder.
Hauser [14] previously observed that an inability of the musculature of the back to perform up to the requirements of the demand will ordinarily produce an increase in all the normal curves of the spine. He attributes this to the functional adaptation of the spine, with a subsequent muscular imbalance between the anterior and posterior structures. This subsequently produces an increase in the anterior and posterior curves, recognized as "poor posture."
Hauser [14] further reported that if muscular imbalance is uncorrected, a lateral curvature may develop, ultimately producing a compensatory structural scoliotic development. He concluded that whenever there is a decrease in strength of the structure of the back, or loss of capacity. or if there is an increase in the demand made on the back, such as an overload, or a combination of the two exists, scoliosis will develop. If the occurrence of lateral, and anterior and posterior curvatures are combined, the spine will be subject to increasing stress, if it is exposed to torsional rotation.
Krahl and Steinbruck [17] noted unilateral upper limb motion in athletics is a torsional repetitive motion. This occurs in combination with trunlt rotation, owing to strong pectoralis contraction such as that required in the freestyle, which therefore represents a considerable etiologic development in swimmers’ scoliosis.
Studies of trunk muscular strength in scoliosis are mixed in indicating this area as a sole source of causative stresses. Eckerson and Asclgaard [11] found lateral electrical stimulation of trunk musculature may be effective in reducing the degree of scoliotic curvature in humans, after having artificially induced scoliosis in cuts by a similar method.
Portillo et. all. [13] in research on the trunk strengths of normal and idiopathic scoliotic adolescent girls, reported no significant diflercnces in lateral flexion, flexion, or extension. This latter study was conducted on patients with mild lateral curves, who had to date been untreated by exercise or bracing. The results of this investigation, when compared with biopsy studies [27, 36] showing definite histologic and morphologic changes at either side of the curve, were interpreted as being due to the advanced cases of scoliosis selected for surgical intervention. From this information, the authors suggested the etiology of the scoliotic curve had yet to be determined, and trunk strengths were not a causative factor.
DEVELOPMENT OF SCOLIOTIC CURVATUBE
The presence of scoliosis among preadolescent and adolescent swimmers may be indicative of motor development patterns having a direct relationship on the skeletal growth of the vertebrae. Research by Risser and Ferguson [25] has shown the spine grows slowly from 7 to 10 years of age, and three to live degrees of curvature may develop each year during that period.
The preadolescent age of 10 to 15 years is a period of rapid growth, and curvature increases may develop as quickly as one degree per month. Additional evidence of this age group being a primary population for alteration in vertebral growth has been provided by Zaousais and James [36], and Risser [25], who noted spinal growth in girls stops at an average age of 14.5 years and at 16.5 years for boys. This would be considered a primary age for obvious scoliotic developments among the many swimmers who have followed prolonged training in order to reach high levels of competition.
It may be assumed that the repetitive exercise motions required in swimming that produce physiologic adaptations, as noted by Lavoie, Taylor, and Montpetit [19], are also capable of producing muscular adaptation and thus a contracted spinal curve.
Tachdjian [36] indicated muscle power of the patient with scoliosis should be examined, in the anterior and lateral abdominals, erector spinae, quadratus lumborum, and thoracic groups. He found this to be required because of the possibility that weakened muscle groups may be an area where unequal upper extremity strength would cause a considerable torsional force, resulting in the scoliotic spine.
SWIMMING AS REHABILITATION FOR SCOLIOSIS
The irony of the incidence among swimmers is the recommendation by Kuprian, Ork, and Meissner [18], and Tachdjian [30] that swimming is considered the most excellent exercise in the rehabilitation program, because of the need to incorporate a direct breathing technique that prevents thoracic damage. Kuprian, Ork, and Meissner [18] do, however, state all exercises and movements that compress the spine, or require frequent repetition of torsion and sideward motion, should be avoided by the scoliotic patient. These are precisely the motions required of the upper extremity and spine during the performance of the swimming activity.
Коротко и по-русски: Куприан, Орк и Мейснер утверждают, что все упражнения и движения, которые сжимают позвоночник или требуют частого повторения вращений (поворотов) и наклонов должны ИЗБЕГАТЬСЯ для пациентов со сколиозом. Это именно те движения верхних конечностей и позвоночника, которые требуются во время плавательной активности.
(Ещё раз: движение с подниманием или закидыванием руки выше головы СЖИМАЕТ верхнегрудной и шейный отделы позвоночника - H.B.)
In cases of stroke technique error that are often seen among novice competitive swimmers and untrained recreational swimmers, there is a high incidence of unilateral trunk rotation and lateral sway. In many instances, these types of stroke errors in swimming technique can be responsible for the unequal development of the upper extremity girdle and thoracic musculature.
The functional scoliosis that is prevalent in swimmers often is accompanied by overdevelopment of one upper extremity, similar to the athletic scoliosis noted by Kuprian [18]. Among athletes whose sports require extreme unilateral upper extremity torque and repetitive motions, it is questionable whether swimming is the activity of choice for scoliosis rehabilitation programs.
Cobb [7], Keim [16], Kuprian [18], Roaf [26], and Tarr [31] do not believe that exercise of ANY kind is beneficial to inhibiting the scoliotic development.
In 1941 the American Orthopedic Association Research Committee came to the conclusion, after a study of 425 cases of end-result idiopathic scoliosis, that exercise should be avoided. This study found that approximately 60 per cent of the patients treated with exercise had an increase in the deformity, and 40 per cent had no change.
The support by Blount and Moe [5], Adams [1], and others [18, 30] for swimming as a scoliotic treatment is seemingly contradicted for the potential effects that may be imparted on the musculoslceletal system.
CONCLUSION
The evidence available for definite conclusions regarding the incidence of scoliosis among swimmers remains to be totally convincing, and the cause of the problem has yet to be determined. It is, however, obvious that the repetitive swimming activity will definitely cause adaptation of the primary structures and musculature, with the possibility that a secondary adaptation can occur in the vertebral structure. Although there has been no conclusive evidence to support the role hormonal development has
played in the scoliotic curvature, the incidence among adolescents and preadolescents encourages study in this area. In addition, biomechanical assessment of stroke technique among swimmers should be an area of investigation, owing to the high incidence of mild curvatures, to determine if kinesthetics and/or hand dominance play a role in the etiology of scoliosis in swimmers.
The role of swimming as a therapeutic exercise in the treatment of scoliosis is definitely contraindicated, based on studies that show exercise has little eflect on the reversal of the curvature. It is therefore assumed that competitive swimming may have a progressive effect on the curvature, if the athlete is training during the adolescent ages of 10 to 15 years.
Коротко и по-русски: Вывод. Плавание при лечении сколиоза определённо противопоказано, основываясь на исследованиях, которые показывают, что упражения не имеют эффекта на выпрямление искривления.
Таким образом, соревновательное плавание может иметь прогрессирующий эффект на искривление, если спортсмен(ка) тренируется в возрасте от 10 до 15 лет.
Although there are many factors that may contribute to the cause of scoliosis in swimmers, there is major evidence to indicate the mechanics of the strokes and the subsequent muscular adaptation due to the training can be significant contributors to the onset of scoliosis.
REFERENCES
1. Adams, R.C., Daniel, A. N., McCubbin. J. A . et al.: Games. Sports and Exercises for the Physically Handicapped. Philadelphia, Lea & Febiger, 1982.
2. American Orthopedics Association Research Committee Report. End-result study of the treatment of idiopathic scoliosis. J. Bone Joint Surg., 23A: 963, 1941.
3. Arkin, A. M.: The mechanism of the surgical changes in scoliosis. J. Bone Joint Surg., 31A: 5l9, 1949.
4. Avikainen, V. J., and Vaherto, H.: A high incidence of spinal curvature. Acta Orthop. Scand., 54: 267-273, l983.
5. Blount, W. P. and Moe, J.H.: The Milwaukee Brace. Baltimore. Williams & Wilkins Co., 1978.
6. Clarys, J. P.: A review of EMC in swimming: Explanation of facts and/or feedback information. In Hollander, A. P., Huijing, P. A., and de Groot. G. (eds.): Biomechanics and Medicine in Swimming, Champaign, Illinois, Human Kinetics, 1983.
7. Cobb, J. R.: Scoliosis. J. Bone Joint Surg., 40A: 510, 1958.
8. De Smet, A. A., Asher. M. A., Cook. L. T., et al.: Three-dimensional analysts of right thoracic idiopathic scoliosis. Spine. 9: 377, 1984.
9. Deaver, G. C., and Coulter. J. S.: Physical medicine applied to swimming. Athletic J., 13(5): 30, 1933.
10. Dendy, J. M., Chase, S., and Detemann, P.: School screening for scoliosis. Physiotherapy, 69(7): 272, 1983.
11. Eckerson, L. F., and Axelgaard, J.: Lateral electrical surface stimulation as an alternative to bracing in the treatment of idiopathic scoliosis. Phys. Ther., 64: 483, 1984.
12. Fisher, R. L., and DeGeorge, F. V.: Idiopathic scoliosis: An investigation of genetic and environmental factors. J. Bone Joint Surg., 49A: l005, 1967.
13. Gallenstein, J., and Huston, R. L.: Analysis of swimming motions. Human Factors, 15: 91-98, 1973.
14. Hauser, E.: Scoliosis. Physiother. Rev., 17(6): 234-239, 1937.
15. Jensen, R. K., and Bellow, D. G.: Upper extremity contraction moments and their relationship to swimming training. J. Biomechanics, 9: 219-225, 1976.
16. Keim, H. A.: The Adolescent Spine. New York, Springer-Verlag, 1982.
17. Krahl, H., and Steinbruck, K.: Sportsachaden and Sportverletzungen and der Wirbelsaule. Deutsch Arztebl., 19, 1978.
18. Kuprian, W.: Physical Therapy for Sports. Philadelphia, W. B. Saunders Co., 1982.
19. Lavoie, J., Taylor, A. W., and Montpetit, R. P.: Physiological effects of training in elite swimmers as measured by a free Swimming test. J. Sports Med., 21: 38-41, 1981.
20. Maas, G. D.: The shape of the pectoralis major muscle in swimmers. In Clarys, J. P., and Lewillie, L. (eds.): Swimming II. Baltimore, University Park Press, 1975.
21. Magel, J. R, and McArdle, W. D.: Propelling force and metabolic and circulatory considerations in swimming. Scholastic Coach, 40: 58-70, 1970.
22. Piette, G., and Clarys, J. P.: Telemetric EMG of the front crawl movement. In Terauds, J., and Bedingfield, W. (eds.): Swimming Ill. Baltimore, University Park Press, 1979.
23. Portillo, D., Sinkora, G., McNeill, T., et al.: Trunk strengths in structurally normal girls and girls with idiopathic scoliosis. Spine, 7: 551-554, 1982.
24. Risser, J. C.: Clinical evaluation of scoliosis. J.A.M.A., 164: 134-136, 1957.
25. Risser, J. C., and Ferguson, A. B.: Scoliosis. J. Bone joint Surg., 18d: 667, 1936.
26. Roar, R: Paralytic scoliosis. J. Bone joint Surg., 38B: 640-659, 1956.
27. Sahgal, V., Shah, A., Flanagan, N., et al.: Morphologic and morphometric studies of muscle in idiopathic scoliosis. Acta Orthop., 54: 242-251, 1983.
28. Shands, A. R., and Eisberg, H. B.: The incidence of scoliosis in the state of Delaware. Acta Orthop. Scand., 40: 608, 1969.
29. Svec, O. J.: Biofeedback for pulling efficiency. Swim. Tech., 19(1):38-46, 1982.
30. Tachdjian, M. 0.: Pediatric Orthopedics. Philadelphia, W. B. Saunders Co., 1972.
31. Tarr, I.: Analysis of normal and scoliotic spine. Physiother. Rev., 28: 6-10, 1948.
32. Vercauteren, M., Van Beneden, M., Verplaetse, R., et al.: Trunk asymmetries in a Belgian school population. Spine, 7: 555-562, 1982.
33. Webster, F. S.: The problem of scoliosis. Nebr. Med. J., 35: 115, 1951.
34. Willner, S.: Prevalence study of trunk asymmetries and structural scoliosis in 10-year-old school children. Spine, 9: 644-647, 1984.
35. Wynne-Davies, R.: Familial (idiopathic) scoliosis. J. Bone joint Surg., 50B: 24, 1968.
36. Yarom, R., Wolf, E., and Robin, G. C.: Deltoid pathology in idiopathic scoliosis. Spine, 7: 453-460, 1982.
37. Yeater, R. A., Martin, R. B., White, M. K., et al.: Tethered swimming forces in the
crawl, breast and back strokes and their relationship to competitive performance. J. Biomech., 14: 527-537, 1981.
38. Zaousais. A. L., and James, J. I.: The iliac apophysis and the evolution of curves in scoliosis. J. Bone Joint Surg., 40B: 422, 1958.
39. Zetterberg, C., Bjork, R., Andersson, G., et a.l.: Quantitative back muscle electromyography in idiopathic scoliosis. In Matsui, H., and Kobayashi, K. (eds.): Biomechanics VIII-A. Champaign, Illinois, Human Kinetics, 1983.
Fankhauser Orthopedic and Sports Rehabilitation
3732 Colby Avenue
Everett, Washington 98201
http://healthy-back.livejournal.com/95378.html?thread=2138258#t2138258
Anonymous
Я занимался плаваньем с того момента как у меня начал прогрессировать сколиоз (2010 год, лето , 2* левосторонний С - обрзный , грудной) Плавал брасс, спина брассом. Симетрично .
вот сейчас такие результаты. Мне 17 (почти 18) лет, у меня S-образный сколиоз 10* обе дуги... грудопоясничный.
Scoliosis in Swimmers
Theodore. Becker, Ph.D" R.P.T., A.T.C'* (Member of the United States Swimming Sports Medicine Committee Executive Council and International Teams Staff 149CLinics in Sports Medicine-Vol. 5, No. I, January 1986)
Children who become interested in swimming and begin to participate seriously often do so at very early ages, sometimes as young as six or seven. This early involvement very often exposes them to types of stress that can affect the growth and development of their maturing musculoskeletal systems in an adverse way, producing a disruption of the normal growth pattern, The most potentially serious of these growth disorders is scoliosis of spinal curvature, because it may deform the body and inhibit normal bodily organ function.
FUNCTIONAL AND STRUCTURAL SCOLIOTIC CURVATURE
The vertebral curvature that is defined as scoliosis has been broadly categorized as either structural or functional. The structural curvature category has been described by Willner [34] Hauser [14] and Portillo [23] as being a deviation of over 10 degrees, accompanied by rotation. This definition specifies the inclusion of bone and ligament malfunction as a criterion for structural torsion associated with a lateral curvature.
Functional scoliosis has been referred to by Keim [16] as a "mild" form of the vertebral disorder, because it is not necessary to correct the condition by an external device, but rather it can be corrected by side bending.
Arkin [3] further noted that the functional or mild curve may in some cases be an initiating cause of the more severe structural curvature, but it is notably a postural fault for which correction is possible without surgery.
Tachdjian [30] noted that functional scoliosis generally has a single long thoracolumbar curve with a predominately left convexity. His work indicates functional scoliosis produces little rotation of the vertebral body with accompanying rib deformity, which is the serious secondary complication of idiopathic scoliosis.
One of the characteristics of functional scoliosis is that the curve will disappear during recumbency and suspension, and the spine bends equally well to both sides on lateral flexion of the trunk, with rotation to both sides being equal. According to Tachdjian [30] the majority of functional scoliosis cases are attributable to compensatory lower limb growth, or compensatory pelvic tilt adjustments affecting the lumbosacral junction. Some degree of functional scoliosis is a common occurrence with poor posture, but this entity is of little clinical importance and ordinarily requires no treatment.
INCIDENCE OF SCOLIOSIS
The incidence of idiopathic structural scoliosis has been normally low among the general population, but is notably higher among adolescents. In a 1955 survey of 50,000 adolescents in the general population, Shands and Eisberg [28] found 1.9 per cent or approximately 1000 subjects to have scoliosis. Avikainen and Vaherto [4] in 1983 reported scoliosis to be present in 3 to 16 per cent of the population, depending on the degree of curvature that had been chosen as the limit of scoliosis, and on the age of the subject. These percentages are similar to the findings of Willner [34] who in 1984 reported 0.35 to 13 per cent as the incidence ofstructural scoliosis. Eckerson and Axelgaard [ll] in 1984 also reported that idiopathic scoliosis, with a lateral curvature of unknown etiology, comprises 75 to 80 per cent of all scoliosis in the United States.
Studies focusing on the incidence among men and women include the work of Shands and Eisberg [28], which showed a predominance among women; the incidence of scoliosis may be five times as great as that found in like male population.
Avikainen and Vaherto [4] report in all cases of scoliosis requiring treatment, 90 per cent are women, but mild scoliosis observed to be nearly as frequent in boys as in girls. Other investigations by Wynne-Davies [36] and Fisher and DeGeorge [12] surveyed familial incidence of scoliosis and the relationship to mothers’ age. These studies showed a significantly greater than expected number of scoliotic curvatures among the offspring of mothers who were considered to be older. In additional investigations, Yarom, Wolf, and Robin [27] indicated that growth and sex hormones and scoliotic onset later in life may be decisive factors in the propagation of the deformity.
Further work on the incidence of scoliosis reported by Kuprian, Ork, and Meissner [18] indicates that Jenschura found the average frequency if idiopathic scoliosis in athletes to be 2 per cent. Krahl and Steinbruck [17] in examining 571 top athletes in 1974-1977, found a 33.5 per cent incidence of functional scoliosis and a 1.6 per cent incidence of idiopathic scoliosis, similar to the incidence noted by Shands and Eisberg [28]. Kuprian, Ork, and Meissner [18] postulated that the high incidence of functional scoliosis among athletes is notable among those participating in sports that develop extreme torque in repetitive serving, throwing, and volleying motions, such as archers, javelin throwers, pole vaulters, and table tennis players.
Figure 1. A and B Athletes screened for scoliosis were observed in the standing erect position for asymmetries of the lateral contours of the trunk, shoulders, and scapulae.
The clinically observed scoliosis in swimmers does present the aquatic sports physician and therapist with a potentially interesting investigation as to etiology and incidence. Owing to the great number of adolescents engaged in competitive swimming programs each year, a preliminary study was conducted to ascertain the incidence of scoliosis among this group. In August of 1983, at the Junior Olympic Swimming Championships East, held at the Indiana University Natatorium, Indianapolis. 836 of 1200 competitors underwent evaluative screening for scoliosis. The procedure was patterned after the protocol of Dendy, Chase, and Determann [10], Risser [24], and Willner [34]. This screening procedure included observations with the athlete in the standing erect position, and then in the forward bending position. In the standing erect position, observations were made for asymmetries of the lateral contours of the trunk (Fig 1), shoulders, scapulae, and the lateral deviation of the spinal processes (Fig. 2).
Figure 2. A and B. Swimmers screened for scoliosis were also observed for lateral deviation of the spinal processes.
Of the 336 athletes who participated, 198 females and 173 males, 6.9 per cent were found to have structural idiopathic signs in each group. Each of these groups was found to have a 16 per cent incidence of mild functional scoliosis. The 6.9 per cent figure represents an incidence that is three and one half times the normal incidence, and is well above the 1.9 per cent figure in other studies [17, 28], whereas the 16 per cent is similar to the high figures of Avikainen and Vaherto and of Willner [34] yet below the 33.5 per cent figure of Krahl and Steinbruck [17].
The screening investigation at the Junior Olympic Swimming Championships East, in which 16 per cent were noted to have mild functional curvatures, did produce a unique statistic. In this study the 16 per cent figure included a 100 per cent occurrence of lateral curvature to the hand-dominant side of the body. This supports the muscular imbalance according to Hauser [14], and the dominant arm strength as noted by Yeater et. al. [37], as possible contributors to these particular investigations.
Figure 3. In the forward bending position, observation of rib hump asymmetry was considered to be a positive clinical finding for a structural idiopathic scoliosis.
In the forward bending position, the observed rib hump asymmetry was considered to be the positive clinical finding for structural idiopathic scoliosis (Fig. 3).
It is obvious that the incidence in this small population is of interest to the swimming community, owing to the fact that the event at which the screening clinic was conducted is noted to be a select event. Competitors were entered based on their being capable of swimming at an acceptable level prior to entry, thus placing this population in an elite category, similar to those athletes studied by Krahl and Steinbruck [17].
INTRINSIC EFFECTS OF SWIMMING
It has been stated by Magel and McArdle [21] that the propeling force in swimming depends on muscular strength and eflective stroke mechanics. Swimming speed increases depend in part on buoyancy (плавучесть), the hydrodynamics of correct stroke technique, and wave-making resistance. The propulsive force must equal water resistance, and swimming velocity will result from the relative equilibrium found between force and resistance.
Piette and Clarys [22] electromyographic data revealed the muscles most responsible for the propulsion of the competitive swimmer were the latissimus dorsi, rectus abdominis, gluteus maximus, biceps brachii, and pectoralis. Their investigation revealed the latissimus dorsi, rectus abdominis, and gluteus maximus were the most active muscles during the freestyle stroke. Results of the study showed that competitive swimmers tested had significantly greater propulsion on electromyography than a like number of noncompetitive swimmers. This study also found the muscular efforts of competitive swimmers were significant for the level of activity in the back, abdominals, and muscles of the pelvic girdle.
In succeeding electromyographic studies, Clarys [6] again investigated the latissimus dorsi and rectus abdominis muscles and the results confirmed these to be the most active in duration and strength during the freestyle of all the muscles investigated.
Propulsive efficiency studies by Svec [29] examining the freestyle stroke note the first state of the arm motion produces a pressure curve that is very close to linear from the point of hand entry and pull (Fig. 4A) through to the initial inward scull (Fig. 4B).
Figure 4. In the freestyle stroke, the first stage of arm motion produces a pressure curve that is very close to linear from the point of hand entry and pull (A) through to the inward scull (B).
The second phone of the stroke, in which pressure curves are greatest, occurs during the last stage of propulsion, when the hand passes the level of the mid chest in the push (C) and finishes in an outward skull phase (D).
The second phase of the stroke, in which pressure curves are greatest, occurs during the last stage of propulsion, in which the hand passes mid chest in the push (Fig. 4C) and finishes in an outward scull phase (Fig. 4D).
High pressure during the propulsive phase of freestyle is almost always present with a duration that is considered to be variable. Yeater et al. [37] in examining the force traces for the crawl stroke, observed that many individuals consistently produced greater peak force with one arm or the other during all phases of propulsion. Quantification of the stroke asymmetry in this study was performed by dividing the right-left differences in peak force by mean peak force, and no appreciable correlation was found between this variable, as well as mean tether force, and competitive velocity.
In another study on the analysis of swimming motions, Gallenstein and Huston [13] found there are dips in the output velocity for all strokes, owing to upper extremity work. Freestyle kicking was noted to produce relatively small changes in the overall freestyle propulsion, and therefore the effort of the upper extremities was interpreted as being relatively unaffected by the efforts of the lower extremities.
Morphologic studies by Sahgal et al. [27] Yarom, Wolf, and Robin [36] and Tachdjian [30] show there are generalized myopathic changes in the paraspinal and gluteus muscles of individuals with idiopathic scoliosis. The structural skeletal changes would then be expected to be accompanied by secondary adaptation of the supporting vertebral soft tissues. The change in soft tissue function is characterized by Tachdjian [30] and Hauser [14] as being atrophy, weakness, and fibrosis on the convex (выпуклый) side of the spine, and thickening and contractions on the concave (впалый) side. (Ровно наоборот. См. http://healthy-back.livejournal.com/178505.html - H.B.)
Of all muscle types tested, [27, 36] there was significant glycogen content, and the mitochondria were found to be significantly higher on the convex side and in the gluteus, but not on the concave side of the apex, where significantly high Z-band values were found.
The histographic work by Yarom, Wolf, and Robin [36] dealt with analysis of the deltoids and the trapezius and quadriceps muscles. These authors reported no striking morphologic pathology, but results of interest included fewer type I Fibers on the concave side than on the convex side. In several cases, the decline was noticeably marked, and the diameters of the fibers were frequently small or hypotrophic, especially on the concave side.
Fiber distribution and size were shown by Yarom, Wolf, and Robin [36] to be clearly characteristic, with a constant decrease in the deltoids of the concave side for the idiopathic sample. The conclusion that was drawn indicated there may be many factors responsible for the noted changes, including intrinsic and hormonally induced membrane abnormalities.
Muscular adaptation has been the focus of several studies by Mass, [20] and Jensen and Bullow [15]. Maas reported the shape of the pectoralis in swimmers was significantly dilierent than in gymnasts, indicating that the sport activity was functionally specific in relationship to the development of the musculature.
Jensen and Bullow [15] report similar information, with evidence that modeling of drag and inertial forces in the freestyle stroke conceivably provide a suffcient load so as to produce functional changes in the muscles, with an expected increase in the contraction moments. This
research additionally found that the contraction moments largely determined the propulsive force of the shoulder.
Hauser [14] previously observed that an inability of the musculature of the back to perform up to the requirements of the demand will ordinarily produce an increase in all the normal curves of the spine. He attributes this to the functional adaptation of the spine, with a subsequent muscular imbalance between the anterior and posterior structures. This subsequently produces an increase in the anterior and posterior curves, recognized as "poor posture."
Hauser [14] further reported that if muscular imbalance is uncorrected, a lateral curvature may develop, ultimately producing a compensatory structural scoliotic development. He concluded that whenever there is a decrease in strength of the structure of the back, or loss of capacity. or if there is an increase in the demand made on the back, such as an overload, or a combination of the two exists, scoliosis will develop. If the occurrence of lateral, and anterior and posterior curvatures are combined, the spine will be subject to increasing stress, if it is exposed to torsional rotation.
Krahl and Steinbruck [17] noted unilateral upper limb motion in athletics is a torsional repetitive motion. This occurs in combination with trunlt rotation, owing to strong pectoralis contraction such as that required in the freestyle, which therefore represents a considerable etiologic development in swimmers’ scoliosis.
Studies of trunk muscular strength in scoliosis are mixed in indicating this area as a sole source of causative stresses. Eckerson and Asclgaard [11] found lateral electrical stimulation of trunk musculature may be effective in reducing the degree of scoliotic curvature in humans, after having artificially induced scoliosis in cuts by a similar method.
Portillo et. all. [13] in research on the trunk strengths of normal and idiopathic scoliotic adolescent girls, reported no significant diflercnces in lateral flexion, flexion, or extension. This latter study was conducted on patients with mild lateral curves, who had to date been untreated by exercise or bracing. The results of this investigation, when compared with biopsy studies [27, 36] showing definite histologic and morphologic changes at either side of the curve, were interpreted as being due to the advanced cases of scoliosis selected for surgical intervention. From this information, the authors suggested the etiology of the scoliotic curve had yet to be determined, and trunk strengths were not a causative factor.
DEVELOPMENT OF SCOLIOTIC CURVATUBE
The presence of scoliosis among preadolescent and adolescent swimmers may be indicative of motor development patterns having a direct relationship on the skeletal growth of the vertebrae. Research by Risser and Ferguson [25] has shown the spine grows slowly from 7 to 10 years of age, and three to live degrees of curvature may develop each year during that period.
The preadolescent age of 10 to 15 years is a period of rapid growth, and curvature increases may develop as quickly as one degree per month. Additional evidence of this age group being a primary population for alteration in vertebral growth has been provided by Zaousais and James [36], and Risser [25], who noted spinal growth in girls stops at an average age of 14.5 years and at 16.5 years for boys. This would be considered a primary age for obvious scoliotic developments among the many swimmers who have followed prolonged training in order to reach high levels of competition.
It may be assumed that the repetitive exercise motions required in swimming that produce physiologic adaptations, as noted by Lavoie, Taylor, and Montpetit [19], are also capable of producing muscular adaptation and thus a contracted spinal curve.
Tachdjian [36] indicated muscle power of the patient with scoliosis should be examined, in the anterior and lateral abdominals, erector spinae, quadratus lumborum, and thoracic groups. He found this to be required because of the possibility that weakened muscle groups may be an area where unequal upper extremity strength would cause a considerable torsional force, resulting in the scoliotic spine.
SWIMMING AS REHABILITATION FOR SCOLIOSIS
The irony of the incidence among swimmers is the recommendation by Kuprian, Ork, and Meissner [18], and Tachdjian [30] that swimming is considered the most excellent exercise in the rehabilitation program, because of the need to incorporate a direct breathing technique that prevents thoracic damage. Kuprian, Ork, and Meissner [18] do, however, state all exercises and movements that compress the spine, or require frequent repetition of torsion and sideward motion, should be avoided by the scoliotic patient. These are precisely the motions required of the upper extremity and spine during the performance of the swimming activity.
Коротко и по-русски: Куприан, Орк и Мейснер утверждают, что все упражнения и движения, которые сжимают позвоночник или требуют частого повторения вращений (поворотов) и наклонов должны ИЗБЕГАТЬСЯ для пациентов со сколиозом. Это именно те движения верхних конечностей и позвоночника, которые требуются во время плавательной активности.
(Ещё раз: движение с подниманием или закидыванием руки выше головы СЖИМАЕТ верхнегрудной и шейный отделы позвоночника - H.B.)
In cases of stroke technique error that are often seen among novice competitive swimmers and untrained recreational swimmers, there is a high incidence of unilateral trunk rotation and lateral sway. In many instances, these types of stroke errors in swimming technique can be responsible for the unequal development of the upper extremity girdle and thoracic musculature.
The functional scoliosis that is prevalent in swimmers often is accompanied by overdevelopment of one upper extremity, similar to the athletic scoliosis noted by Kuprian [18]. Among athletes whose sports require extreme unilateral upper extremity torque and repetitive motions, it is questionable whether swimming is the activity of choice for scoliosis rehabilitation programs.
Cobb [7], Keim [16], Kuprian [18], Roaf [26], and Tarr [31] do not believe that exercise of ANY kind is beneficial to inhibiting the scoliotic development.
In 1941 the American Orthopedic Association Research Committee came to the conclusion, after a study of 425 cases of end-result idiopathic scoliosis, that exercise should be avoided. This study found that approximately 60 per cent of the patients treated with exercise had an increase in the deformity, and 40 per cent had no change.
The support by Blount and Moe [5], Adams [1], and others [18, 30] for swimming as a scoliotic treatment is seemingly contradicted for the potential effects that may be imparted on the musculoslceletal system.
CONCLUSION
The evidence available for definite conclusions regarding the incidence of scoliosis among swimmers remains to be totally convincing, and the cause of the problem has yet to be determined. It is, however, obvious that the repetitive swimming activity will definitely cause adaptation of the primary structures and musculature, with the possibility that a secondary adaptation can occur in the vertebral structure. Although there has been no conclusive evidence to support the role hormonal development has
played in the scoliotic curvature, the incidence among adolescents and preadolescents encourages study in this area. In addition, biomechanical assessment of stroke technique among swimmers should be an area of investigation, owing to the high incidence of mild curvatures, to determine if kinesthetics and/or hand dominance play a role in the etiology of scoliosis in swimmers.
The role of swimming as a therapeutic exercise in the treatment of scoliosis is definitely contraindicated, based on studies that show exercise has little eflect on the reversal of the curvature. It is therefore assumed that competitive swimming may have a progressive effect on the curvature, if the athlete is training during the adolescent ages of 10 to 15 years.
Коротко и по-русски: Вывод. Плавание при лечении сколиоза определённо противопоказано, основываясь на исследованиях, которые показывают, что упражения не имеют эффекта на выпрямление искривления.
Таким образом, соревновательное плавание может иметь прогрессирующий эффект на искривление, если спортсмен(ка) тренируется в возрасте от 10 до 15 лет.
Although there are many factors that may contribute to the cause of scoliosis in swimmers, there is major evidence to indicate the mechanics of the strokes and the subsequent muscular adaptation due to the training can be significant contributors to the onset of scoliosis.
REFERENCES
1. Adams, R.C., Daniel, A. N., McCubbin. J. A . et al.: Games. Sports and Exercises for the Physically Handicapped. Philadelphia, Lea & Febiger, 1982.
2. American Orthopedics Association Research Committee Report. End-result study of the treatment of idiopathic scoliosis. J. Bone Joint Surg., 23A: 963, 1941.
3. Arkin, A. M.: The mechanism of the surgical changes in scoliosis. J. Bone Joint Surg., 31A: 5l9, 1949.
4. Avikainen, V. J., and Vaherto, H.: A high incidence of spinal curvature. Acta Orthop. Scand., 54: 267-273, l983.
5. Blount, W. P. and Moe, J.H.: The Milwaukee Brace. Baltimore. Williams & Wilkins Co., 1978.
6. Clarys, J. P.: A review of EMC in swimming: Explanation of facts and/or feedback information. In Hollander, A. P., Huijing, P. A., and de Groot. G. (eds.): Biomechanics and Medicine in Swimming, Champaign, Illinois, Human Kinetics, 1983.
7. Cobb, J. R.: Scoliosis. J. Bone Joint Surg., 40A: 510, 1958.
8. De Smet, A. A., Asher. M. A., Cook. L. T., et al.: Three-dimensional analysts of right thoracic idiopathic scoliosis. Spine. 9: 377, 1984.
9. Deaver, G. C., and Coulter. J. S.: Physical medicine applied to swimming. Athletic J., 13(5): 30, 1933.
10. Dendy, J. M., Chase, S., and Detemann, P.: School screening for scoliosis. Physiotherapy, 69(7): 272, 1983.
11. Eckerson, L. F., and Axelgaard, J.: Lateral electrical surface stimulation as an alternative to bracing in the treatment of idiopathic scoliosis. Phys. Ther., 64: 483, 1984.
12. Fisher, R. L., and DeGeorge, F. V.: Idiopathic scoliosis: An investigation of genetic and environmental factors. J. Bone Joint Surg., 49A: l005, 1967.
13. Gallenstein, J., and Huston, R. L.: Analysis of swimming motions. Human Factors, 15: 91-98, 1973.
14. Hauser, E.: Scoliosis. Physiother. Rev., 17(6): 234-239, 1937.
15. Jensen, R. K., and Bellow, D. G.: Upper extremity contraction moments and their relationship to swimming training. J. Biomechanics, 9: 219-225, 1976.
16. Keim, H. A.: The Adolescent Spine. New York, Springer-Verlag, 1982.
17. Krahl, H., and Steinbruck, K.: Sportsachaden and Sportverletzungen and der Wirbelsaule. Deutsch Arztebl., 19, 1978.
18. Kuprian, W.: Physical Therapy for Sports. Philadelphia, W. B. Saunders Co., 1982.
19. Lavoie, J., Taylor, A. W., and Montpetit, R. P.: Physiological effects of training in elite swimmers as measured by a free Swimming test. J. Sports Med., 21: 38-41, 1981.
20. Maas, G. D.: The shape of the pectoralis major muscle in swimmers. In Clarys, J. P., and Lewillie, L. (eds.): Swimming II. Baltimore, University Park Press, 1975.
21. Magel, J. R, and McArdle, W. D.: Propelling force and metabolic and circulatory considerations in swimming. Scholastic Coach, 40: 58-70, 1970.
22. Piette, G., and Clarys, J. P.: Telemetric EMG of the front crawl movement. In Terauds, J., and Bedingfield, W. (eds.): Swimming Ill. Baltimore, University Park Press, 1979.
23. Portillo, D., Sinkora, G., McNeill, T., et al.: Trunk strengths in structurally normal girls and girls with idiopathic scoliosis. Spine, 7: 551-554, 1982.
24. Risser, J. C.: Clinical evaluation of scoliosis. J.A.M.A., 164: 134-136, 1957.
25. Risser, J. C., and Ferguson, A. B.: Scoliosis. J. Bone joint Surg., 18d: 667, 1936.
26. Roar, R: Paralytic scoliosis. J. Bone joint Surg., 38B: 640-659, 1956.
27. Sahgal, V., Shah, A., Flanagan, N., et al.: Morphologic and morphometric studies of muscle in idiopathic scoliosis. Acta Orthop., 54: 242-251, 1983.
28. Shands, A. R., and Eisberg, H. B.: The incidence of scoliosis in the state of Delaware. Acta Orthop. Scand., 40: 608, 1969.
29. Svec, O. J.: Biofeedback for pulling efficiency. Swim. Tech., 19(1):38-46, 1982.
30. Tachdjian, M. 0.: Pediatric Orthopedics. Philadelphia, W. B. Saunders Co., 1972.
31. Tarr, I.: Analysis of normal and scoliotic spine. Physiother. Rev., 28: 6-10, 1948.
32. Vercauteren, M., Van Beneden, M., Verplaetse, R., et al.: Trunk asymmetries in a Belgian school population. Spine, 7: 555-562, 1982.
33. Webster, F. S.: The problem of scoliosis. Nebr. Med. J., 35: 115, 1951.
34. Willner, S.: Prevalence study of trunk asymmetries and structural scoliosis in 10-year-old school children. Spine, 9: 644-647, 1984.
35. Wynne-Davies, R.: Familial (idiopathic) scoliosis. J. Bone joint Surg., 50B: 24, 1968.
36. Yarom, R., Wolf, E., and Robin, G. C.: Deltoid pathology in idiopathic scoliosis. Spine, 7: 453-460, 1982.
37. Yeater, R. A., Martin, R. B., White, M. K., et al.: Tethered swimming forces in the
crawl, breast and back strokes and their relationship to competitive performance. J. Biomech., 14: 527-537, 1981.
38. Zaousais. A. L., and James, J. I.: The iliac apophysis and the evolution of curves in scoliosis. J. Bone Joint Surg., 40B: 422, 1958.
39. Zetterberg, C., Bjork, R., Andersson, G., et a.l.: Quantitative back muscle electromyography in idiopathic scoliosis. In Matsui, H., and Kobayashi, K. (eds.): Biomechanics VIII-A. Champaign, Illinois, Human Kinetics, 1983.
Fankhauser Orthopedic and Sports Rehabilitation
3732 Colby Avenue
Everett, Washington 98201
http://healthy-back.livejournal.com/95378.html?thread=2138258#t2138258
Anonymous
Я занимался плаваньем с того момента как у меня начал прогрессировать сколиоз (2010 год, лето , 2* левосторонний С - обрзный , грудной) Плавал брасс, спина брассом. Симетрично .
вот сейчас такие результаты. Мне 17 (почти 18) лет, у меня S-образный сколиоз 10* обе дуги... грудопоясничный.