NMT IV: Lower Extremities
HIP
only a few maneuvers
very stable joint, capsule is tight, inferior and lateral motion limited
plenty of osteoarthritis, rarely hypermobile
osteopenia dt use of corticosteroids, lack of weight bearing exercise
AVN can occur dt short term corticosteroid use
risk of avascular necrosis dt decr circ foveal artery
even inhaler use may affect bones
pts who do high impact wt bearing or are overwt may need decompression of joint sfcs

TOTAL HIP REPLACEMENT

early rehab very careful
adduction and flexion are limited initially, can make replacement unstable
no crossing legs, can cause dislocation
demented individuals more likely to have trouble with rehab
most people recover very well
femoral head and neck are replaced, acetabulum may also be replaced
titanium and plastic, cement to glue new neck into old femur
capsule is cut, usu lateral approach, leaves zipper scar down side of hip
good amount of blood lost in surgery

INFERIOR GLIDE OF FEMORAL HEAD
duke scoop for assessment and tx
must have 90 degrees flexion ROM
should be tight and springy, not loose or clunky
pt lies supine
got to get body into it
be aware of people's "junk" and avoid it
ask men to move it over if it's in the way
one knee on table and pt leg over my shoulder
pt distal thigh on clavicle
take out slack with inferior pull on double ulnar knife edge
pull direction: inf, inf medial, inf lateral
can stretch the capsule with traction: myofascial release
long axis traction from heel and upper ankle
pull and or oscillate or impulse (grade 5)
can also grasp above knee to traction
can also traction at ankle and move through ROM esp lat
KNEE

INTERNAL AND EXTERNAL ROTATION OF TIBIA
accessory movements
pt supine, hip and knee 90 90
stand beside table, put my foot on table and rest her achilles on my distal thigh
both thumbs on lateral side of tibial tubercle applying torque
fingers above and below
don't dig into stomach 36 point with poky thumbpoints
but hover over it with thumb pads
for lateral rot
put one thumb on medial aspect of tibial tubercle
moves more than hip, springy endfeel, should not be painful
pain: damaged medial meniscus, ligamentous instability
"repairs are a lot more delicate than excisions"
they won't do repairs on inner 1/3 of meniscus, poorly vascularized
outer 3rd well vascularized, middle third intermediate
"surgeons don't like repairs that go south" "ruins their reputation"
ANTERIOR DRAWER
sit on foot, knee at 90
assess ACL
pull behind tibia with thumbs on tibial plateau
if restrx can adjust
POSTERIOR DRAWER
assess PCL
sit on foot, knee at 90
use thenar eminences to push A-P on tib
and sense joint gap with thumbs
normal mvmnt 3-4 mm, past 5 it's hypermobile
check both sides, pt may be hypermobile in general
ask about hx if two abn or one
ANTERIOR AND POSTERIOR GLIDE OF THE FIBULA
non-weight bearing bone should move freely
knee at 90, sit on foot
anterior glide
wrap fingers of both hands around back of fibula
pull forward
posterior glide
use ipsilateral hand, thumb pad on fibular head, fingers on medial tibia
back up pushing thumb with thenar or hypothenar of other

GAPPING THE KNEE
prone, duke scoop p 9
clavicle on pt ankle
knife edge in popliteal fossa, pull there
indic: compression, congestion, decr flexion or other ROM, edema (improve circ)
ANTERIOR GLIDE OF THE FIBULA (PRONE)
capture back of fib
pull and assess with 5th metacarpal
a modified duke scoop, similar but not same

CASE
27yo male with infrapatellar pain x2wks after nt of dancing
tall thin athletic male
presents with swelling and stiffness
point tenderness on medial joint line
basketball injury to same knee, 2 yrs prior, audible pop, untreated
pop = ligement or tendon,
can't do anything last 2 wks
soft positive patellar balottment
sig infrapatellar swelling, not hot
squeaking of tendon with extension/flexion
positive patellar grind bilaterally, pos common in jumpers (basketball) and women
DDX: investigate: MCL and medial meniscus, anterior cruciate
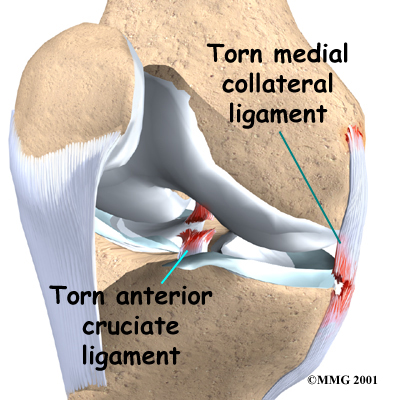
"when one goes check the other two" "not the case on the lateral side"
lateral collateral doesn't share any attachments
valgus stress test reveals hypermobility and pain
soft pos anterior drawer, neg posterior
neg thessaly
pos mcmurray's: click or pop with extension
Tx: conservative

PATELLAR BALOTTEMENT
knee straight
detect when intra-articular swelling elevates patella above femoral condyles
if press on patella and it sinks in there's fluid in the joint
could be dt ACL, PCL, meniscus injury


PATELLAR GRIND
for chondromalacia patella, hyaline under patella worn out
common among young women
tissue behind patella looks like strips of crab meat
patellar tracking problem, tight vastus lateralis and IT band
eliminate uphill climbing to rest it
painful going down hill, pt wants to keep knee straight
tx: strengthen vastus medialis, straight leg raises with leg ext rotated
PATELLAR APPREHENSION
test to see if it will easily dislocate to lateral
CHECK KNEES FOR TRACKING OF PATELLA
bend them and see where the patellae run
assymetry?
OBERS TEST
for tight IT band
HER FAVE TX FOR JOINT INJURIES
hydro therapy to remove swelling
microcurrent to increase ATP production
ultrasound
injection: prolotherapy, glucosamine sulfate
nutrition: MSM, glucosamine chondroitin, zinc, vit C, manganese etc for CT
bvits, prot
diabetics be careful with glucosamine
adverse rxns to MSM ?? dizzy??
appropriate exercise levels
protomorphogens (she has mixed feelings about glandulars)
THESSALY TEST
pt stands on one foot, holds something, bends standing knee 15-20degrees
twist as far as possible in each direction
if the knee is unstable pt will feel it
APPLEYS COMPRESSION
prone
mash it, twist and turn
reveals meniscus
APPLEY'S DISTRACTION
pt prone
anchor pt leg with my knee and pull up on ankle
assesses collaterals and relieves meniscus pain
MCMURRAY'S
supine
max knee flexion
finger on joint line
ext rot foot to palp medial meniscus
hold ext rot and fully extend
pop or click is positive pain is confirmatory
finger on lateral meniscus, fully flex, int rot, hold rot while extend leg
click or pop?